Is Mexico lying about the numbers or is there another reason
I am not a medical expert and this is just a hypothesis; taking BCG vaccination may strengthen immune to the novel coronavirus. If I were American/West European/Australian, I would take BCG vaccination now. Six reasons follow.
I declare that there is no conflict of interest for BCG vaccination but I have a big interest in stopping this pandemic. One of my businesses is an online tourism agency and its sales have dried up!
1) Scientists have started to work on this hypothesis
Can a century-old TB vaccine steel the immune system against the new coronavirus?
https://www.sciencemag.org/news/2020/03/can-century-old-tb-vaccine-steel-immune-system-against-new-coronavirus
The Max Planck Institute (the best German science institution with 33 Novel Prize winners that developed BCG vaccine a century ago)
Immune boost against the coronavirus
https://www.mpg.de/14610776/immune-boost-corona-virus
Some countries, the U.S. and Australia will start a trial to give BCG vaccine to healthcare workers.
https://foreignpolicy.com/2020/03/24/coronavirus-vaccine-health-care-workers-bcg/
2) If you look at the map displaying BCG vaccination policy by country, there seems to be a correlation to the speed of coronavirus spread and its spread among young people.

https://www.researchgate.net/figure/Map-displaying-BCG-vaccination-policy-by-country-A-The-country-currently-has-universal_fig2_50892386A: The country currently has a universal BCG vaccination program.*B: The country used to recommend BCG vaccination for everyone, but currently does not. The year the country stopped it; Spain 1981, Germany 1998, UK and France 2005-2007 etc.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3062527/C: The country never had universal BCG vaccination programs.
*In Portugal the BCG vaccine was mandatory from 1965 to 2017. https://twitter.com/ruipalma79/status/1243304538469273600
The major correlations are;

- The spread speed is fast in Italy and western Europe and the U.S. while the spread speed among Russia, eastern European countries, and Asian countries except Wuhan city is slow.
- In Asian countries, there are few young infected people or almost zero serious cases among young people. However, in western Europe and the U.S., there are cases among young people.*
- In Western Europe, you can compare Italy vs Croatia, Spain vs Portugal**, UK vs Ireland, Sweden vs Norway, ex-West Germany vs ex-East Germany. In the former countries, BCG vaccine is not mandatory while in the latter countries, BCG vaccine is mandatory. Now, you can compare the U.S. and Mexico.
- I live in Tokyo and Brisbane. Though the normal social distance is much longer and less crowded in Brisbane and the government policy is 10 times stricter, the spread speed is faster in Brisbane than in Tokyo.
In Latin America, Ecuador is the only country that never had universal BCG vaccination programs and all the other countries have universal BCG vaccination programs. Total deaths per million, Ecuador: 2, Colombia: 0.08, Peru: 0.3, Brazil: 0.3.
(Added on 29 Mar)
A reader told me there is a pre-print article (not yet certified by peer review)
https://www.medrxiv.org/content/10.1101/2020.03.24.20042937v1
The article has this chart. I believe if we can adjust for the timing of coronavirus spread, the correlation would be even higher.

(Added on 30 Mar)
In the world map above, Canada is in orange and categorized in C: The country never had universal BCG vaccination programs. However, if you look at Canada in http://www.bcgatlas.org/, it seems that Canada had a “routine” BCG vaccination program until 1960s-1970s (Please correct me if I read wrongly). This means people elder 50s mostly vaccinated! This may be the reason why Canada has a low death rate compared with the U.S. And Canada used BCG Tokyo strain.
One more weak fact. In Canada, people elder than the 60s had a BCG vaccine while people younger than 50s had not. Then, look at the age distribution of COVID-19 cases in Canada. Skew to people younger than the 50s?! But infection rate may not vary by age, only hospitalization/ICU/death rate may vary by age. I’m looking for that data and BCG vaccine penetration data by age group for Canada.

* I couldn’t find good stats on this. Only anecdotal news stories. Eg. Greta Thunberg got infected by the novel coronavirus. Well, she is Swedish and born in 2003. Sweden stopped BCG vaccination in 1975.
** Among West European countries that had/have universal BCG vaccination program, Spain and Portugal are (one of) the last countries introduced it in 1965. And Spain is (one of ) the first country to stop it in 1981 and Portugal stopped it in 2017. Portuguese elder than 55 may have a low BCG vaccination rate, which may result in a high death rate than the other western Europe, but probably better than Spain.
3) There are several strains of BCG vaccination and Soviet/Japan/Brazil strains may be the most effective against the novel coronavirus.
This comment by Tiger Paw sounds most plausible regarding the country differences though the article itself is worthless.https://www.japantimes.co.jp/opinion/2020/03/21/commentary/japan-commentary/japan-still-coronavirus-outlier/#comment-4843977551
* The comment was deleted for some reason. The initial idea of this section attributes to Tiger Paw. If I hadn’t read his comment, I would not know there are multiple types of BCG vaccine.
Soviet/Japan strains of BCG vaccination are old-type and similar while Western European stains are recent and different.
Below is a map of German states with confirmed coronavirus cases. You can see the difference between ex-East Germany and ex-West Germany. The density of the population doesn’t explain this much difference.East Germany had used the Soviet strain of BCG vaccination and West Germany had used the Western Europe strain of BCG vaccination and stopped its mandatory vaccination in 1998. The vaccination strains/policies may be the cause of the difference.

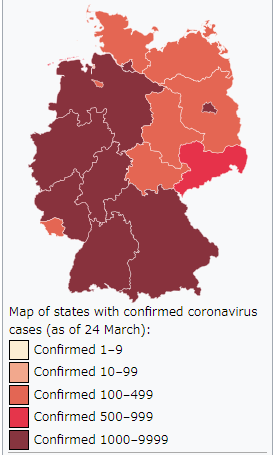
https://en.wikipedia.org/wiki/2020_coronavirus_pandemic_in_Germany
Then, look at the number of deaths by state. Summing up by ex-West Germany and ex-East Germany (excluding Berlin), the number of deaths per 100K of ex-West Germany states is 0.35 while ex-East Germany is 0.11 and Berlin is in between; 0.21 (as of 27 Mar).

I obtained a map showing which strains are used in each country though this map maybe not perfectly correct.
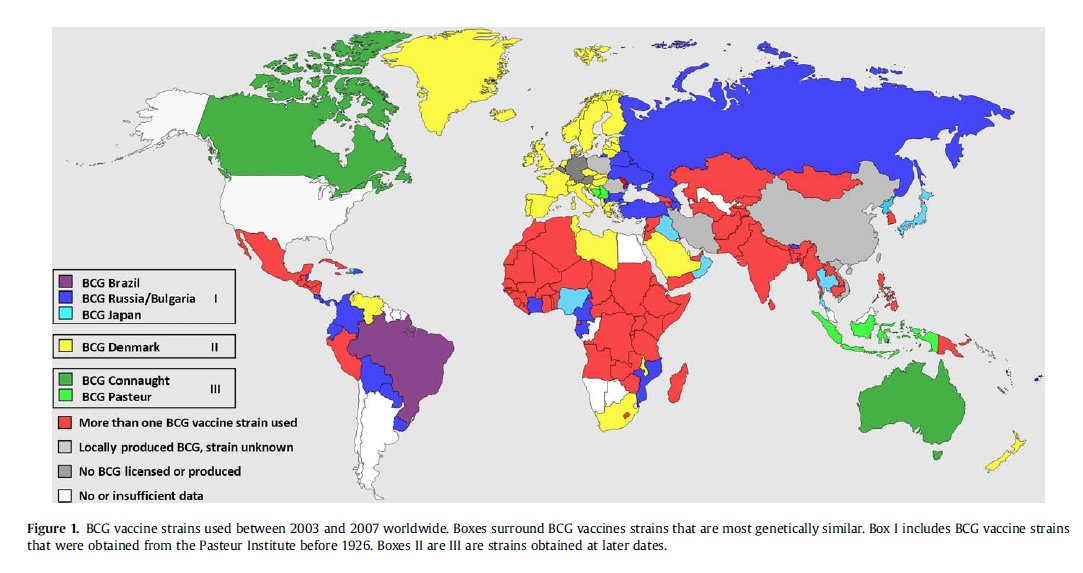
High-level impression; BCG Brazil, BCG Russia/Bulgaria, BCG Japan countries may immune to novel coronavirus. Countries that use more than one BCG vaccine strain look immune, too. BCG Brazil, BCG Russia/Bulgaria, BCG Japan are categorized in “I” and this may be the effective strain category.
Then, I looked into how BCG strains are categorized. I found the chart below. BCG Russia/Japan/Moreau(Brazil) are the first generation of the BCG vaccines.

In the same article, there is a table that shows the differences in each strain character. Though I don’t understand any jargon in the first row, I can see there is quite a difference between BCG Tokyo/Moreau(Brazil)/Russia/Sweden and BCG Copenhagen(Denmark)/Glaxo/Pasteur/Tice. BCG Denmark is the common strain among Western Europe.

While Iraq uses the Japan strain*, Iran uses different strains. According to http://www.bcgatlas.org/ Iran had used its local (original?) BCG vaccine from 1947 to 1984 and make it compulsory in 1984. This means elderly people in Iran have less BCG vaccinated and for those who had it had a local(original?) BCG vaccine. Please check and compare Iraq and Iran figures. You will be surprised to see how different they are.
https://www.worldometers.info/coronavirus/(Iran: 27 deaths per million, Iraq: 0.9 deaths per million as of 27 Mar; added)* Additional source is welcomed. The map above says it BCG Japan but http://www.bcgatlas.org/ does not have Iraq’s strain info. I suspect Iraq uses a different strain.
In Asian countries, China uses a different local produced strain and Korea uses basically BCG Denmark but sometime BCG Japan. Taiwan uses the Japan strain (though the map shows a locally produced strain).
BCG Japan(Tokyo) looks working quite well against the novel coronavirus. 1) Japan, Thailand, Taiwan, and Iraq have used BCG Tokyo and all of them have low death rates though they are close to China or Iran. 2) And so far, it is not reported that any Japanese got severely infected or died in Italy or Western Europe. 3) In Japan, there are 1,349 cases reported, and 934 are Japanese and 415 are non-Japanese. Hmm, quite a high ratio of non-Japanese (as of 28 Mar).
https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000164708_00001.html#kokunaihassei
(Added on 1 Apr)
I am afraid that I hardly understand the mechanism of BCG vaccines but there seems to be a piece of medical evidence that BCG Tokyo works quite well against COVID-19.
https://www.jsatonotes.com/2020/03/if-i-were-north-americaneuropeanaustral.html?showComment=1585702586835#c4287423548330968127
The website, http://www.bcgatlas.org/, seems to have a lot of information about BCG vaccination though this is not perfect, either.
I am afraid that I cannot digest this detailed medical information. Expert explanations will be welcomed.
I live in Tokyo and Brisbane and have been wondering why the spread speed is faster in Australia than Japan.
Tokyo is a very crowded city and it’s impossible to keep the social distance. People are packed in a very crowded train twice a day and I expected a high speed of spread but the actual speed is low so far (though it’s beginning to explode).Here in Brisbane or the other Australian capital cities, the normal social distance is much longer than Tokyo and I expected a slower spread. But the speed of spread is faster.I was wondering about this, and so far this hypothesis may seem to be the most plausible. Maybe ~60% probability.
4) Deaths and severe cases skew to people who probably have not BCG vaccinated.
In Japan and Portugal, the deaths come only to the age group without the mandatory BCG vaccine program period.
In Japan, all babies since 1951 have BCG vaccination and the coronavirus deaths in Japan are skewed drastically to the elderly born before 1951. 44 out of 45 deaths happen to those older than 70 (as of 26 Mar, https://toyokeizai.net/sp/visual/tko/covid19/).
In Portugal, the BCG vaccine was mandatory from 1965 to 2017 (https://twitter.com/ruipalma79/status/1243304538469273600), which means between 3 and 55 years old are vaccinated. And it looks deaths happen only to over 50 (as of 27 Mar, https://www.dgs.pt/em-destaque/relatorio-de-situacao-n-024-26032020-pdf.aspx).

Also, as Portugal introduced the mandatory BCG vaccine program very late together with Spain, in 1965, and there should be many elderly who had not BCG vaccinated, I anticipate that the number of deaths per million will be higher than the other Western European countries where BCG vaccination programs were usually imposed in the 1950s. But Portugal should be better than Spain that stopped the program in 1981, though.
However, this hypothesis is weak since the fatality basically skews to the elderly worldwide. I saw some news that the younger generation became severely ill in Western Europe or the U.S. but have never seen that in Japan. More statistics are required to examine this hypothesis.
(Added on 30 Mar)CDC is publishing hospitalization/ICU/death cases for the U.S. cases. The chart below shows that there are many hospitalizations and ICU cases below 54 years old though the fatality rate is very low so far. (Severe cases may cause aftereffects.) From China case, we know that the fatality rate is very low for the younger generation, which is the same case with the U.S. but the hospitalization/ICU ratio might be higher for the U.S. I cannot find a comparable data regarding hospitalization and ICU cases for China.

Please compare it with the China chart. Very different age distribution. I don’t have good information of China BCG vaccine policy but my guess is that the young Chinese generation probably had a BCG vaccine.

Severe Outcomes Among Patients with Coronavirus Disease 2019 (COVID-19) — United States, February 12–March 16, 2020. MMWR Morb Mortal Wkly Rep 2020;69:343-346. DOI: http://dx.doi.org/10.15585/mmwr.mm6912e2external icon.
(Added on 31 Mar)I received several inquiries regarding China. As there is little data about China’s BCG vaccine policy on http://www.bcgatlas.org/, I had skipped China.
I found three facts regarding China’s BCG vaccine policy.
- China started its BCG vaccination program in 1978 (->42 years old), not universally but partially.
- Penetration varies by province. Among high/middle/low penetration categories, Hubei Province(where Wuhan is) is in the low category. Beijing and Shanghai are in the high category.
- China uses its own local strain produced in China.
This can explain why the death from COVID-19 heavily skews to the elderly, why the spread of COVID-19 varies by province. Well, China strain may be effective against COVID-19 since China controls quite well except Wuhan/Hubei. https://www.huffingtonpost.jp/zhang-qian/compare-vaccine-policy_b_10982252.html
https://www.sciencedirect.com/science/article/pii/S1472979209000262
(Added on 30 Mar)This can be one of the critical supporting facts for this BCG vaccine hypothesis. Below is a death rate of COVID-19 in Spain by age group. You can see a higher death rate in 10s and 20s than the 30s or 40s. Spain had a universal BCG vaccination program from 1965 to 1981, which means from 39 to 55 years old had a BCG vaccine. Well, you can see a little higher rate in the 10s and 20s. It is a very unusual pattern from what we learned from China. Yes, the absolute numbers may be small and not statistically significant. But this is a sign!

5) BCG vaccination has a long history and there seems no little downside to human beings.
BCG vaccination may not work but even in that case, there will be little downside.CDC states the reason it is not recommended in the U.S.https://www.cdc.gov/tb/publications/factsheets/prevention/bcg.htmIn Japan, all babies since 1951 have BCG vaccination and I have not heard a problem with it.
If I were North American/European/Australian, I would take BCG vaccination now.(Added on 28 Mar)I had carefully avoided talking about adult or elderly people to have BCG vaccination again as I don’t know anything about the risk of re-vaccination. But I found a Japanese medical article about re-vaccination to bedridden elderly people published in 2003. BCG re-vaccination significantly reduced the probability of pneumonia.
https://medical.nikkeibp.co.jp/inc/all/hotnews/archives/237265.html
(Added on 31 Mar)Dr. Toshio Hirano, one of the best authorities in immunology, best known for his discovery of interleukin-6, the 17th President of Osaka University, stated that this hypothesis could be right from the perspective of our immune system, citing my blog article.
https://en.wikipedia.org/wiki/Toshio_Hirano
https://www.facebook.com/toshio.hirano.79/posts/2817509081662367
6) Lockdown reduces the reproduction rate significantly but lockdown may not be enough for the countries where BCG vaccination has not been mandatory.
(Added on 1 Apr)
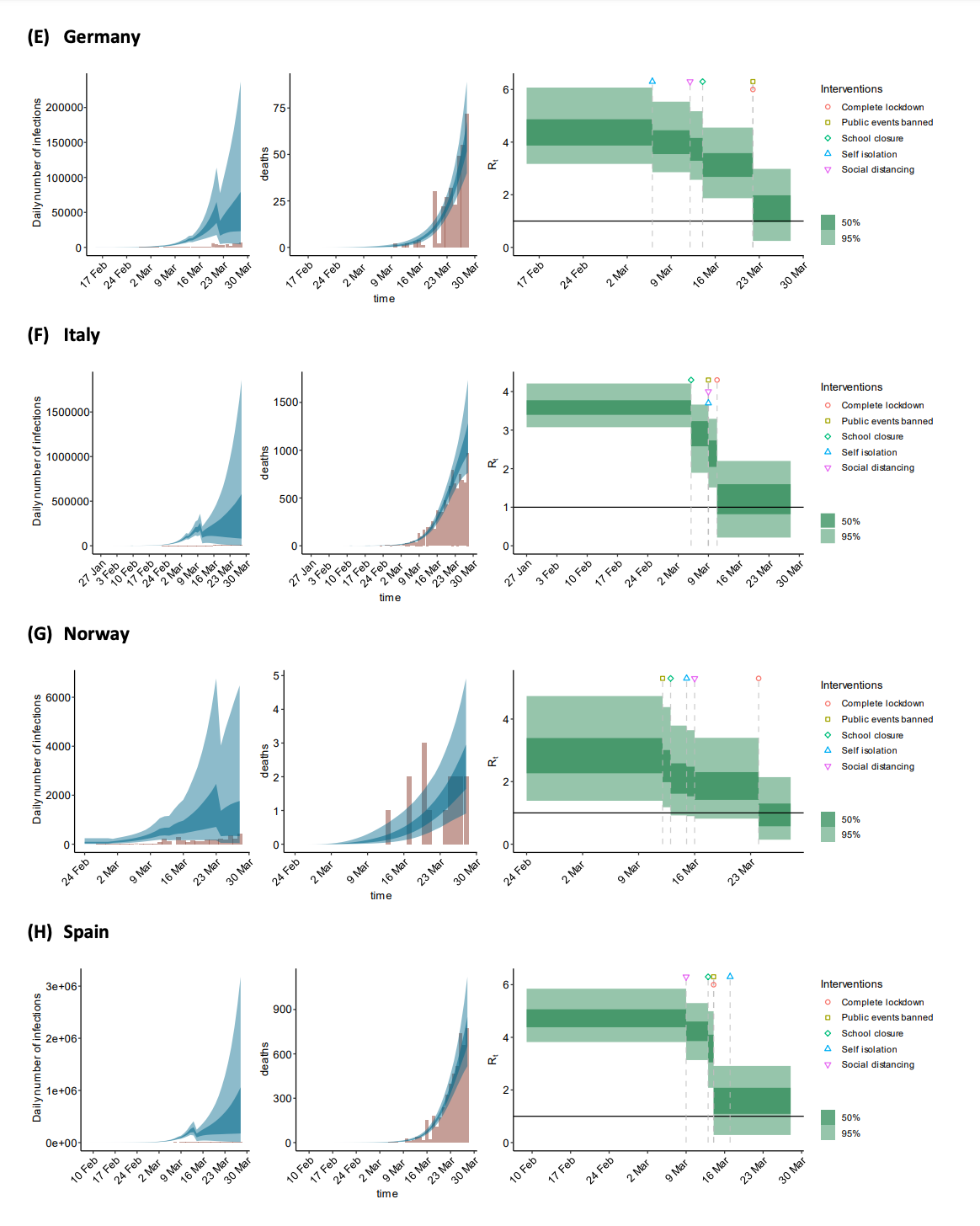
I checked the Imperial College COVID-19 report as of 30 Mar and read the chart of 13 west European countries. I am afraid that I don’t check other than the chart below.
https://www.imperial.ac.uk/media/imperial-college/medicine/sph/ide/gida-fellowships/Imperial-College-COVID19-Europe-estimates-and-NPI-impact-30-03-2020.pdf
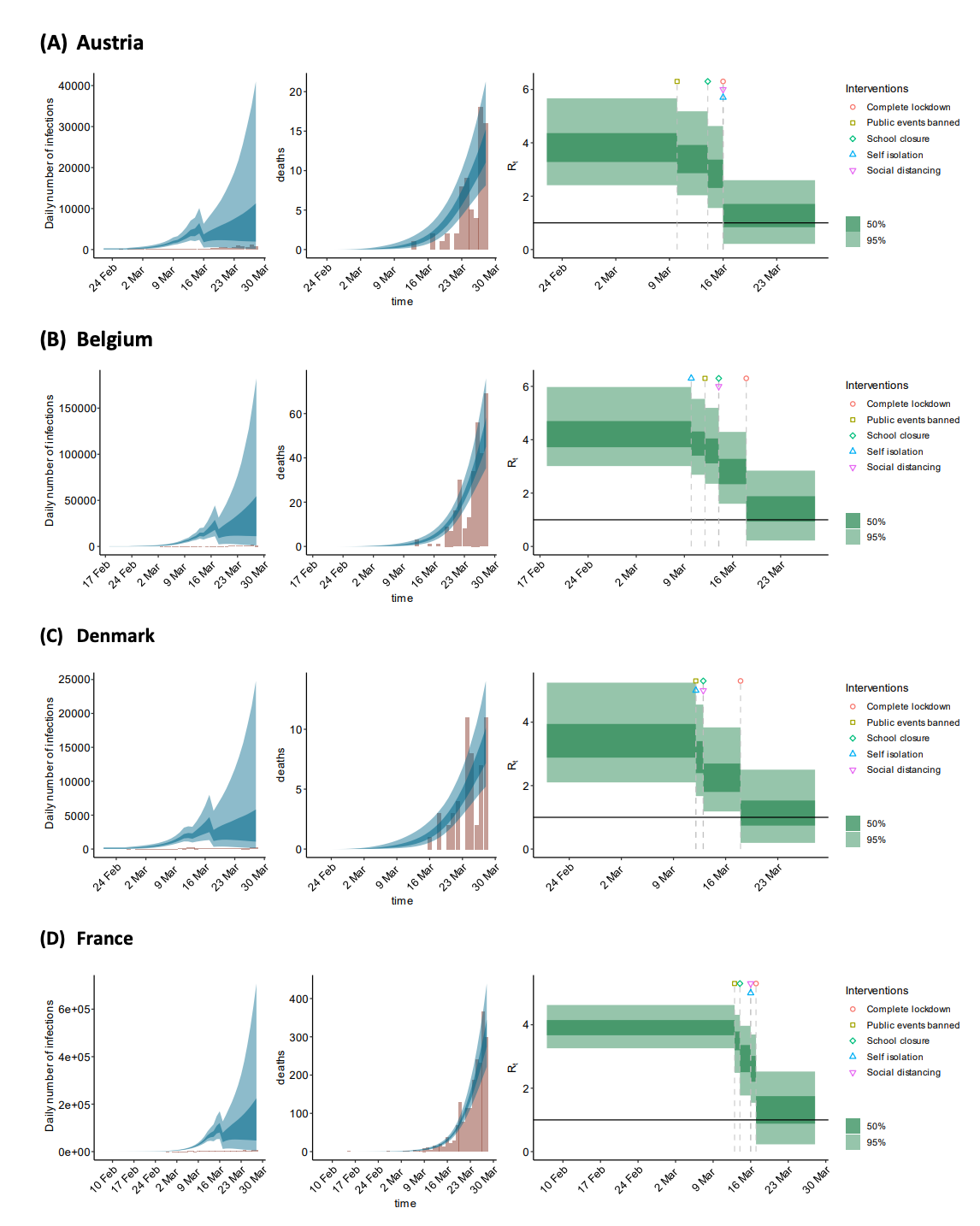
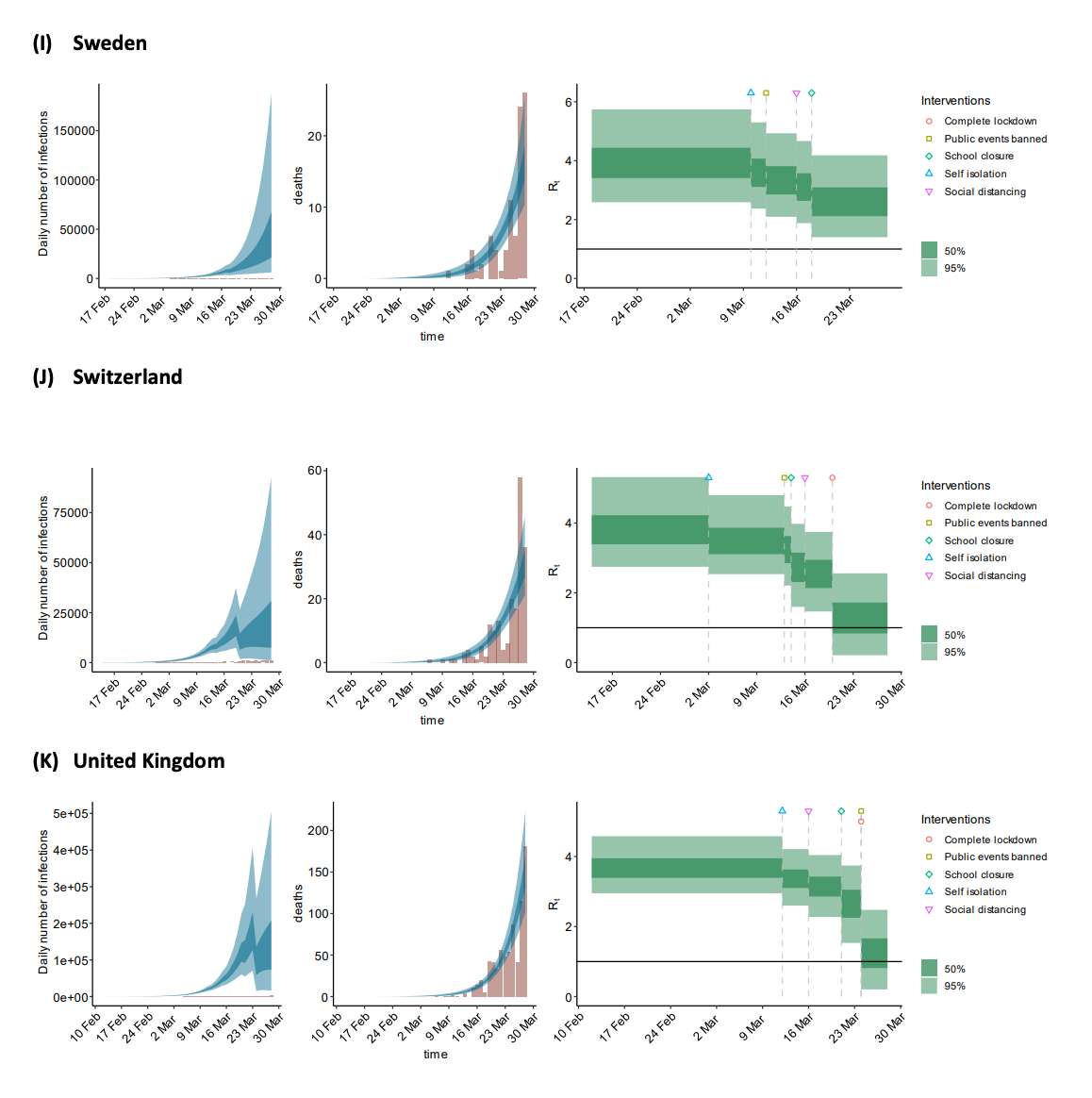
My observation follows;
- 12 out of 13 countries already implemented lockdown and have reduced their R1 significantly. Sweden is the only country not implementing lockdown and making the virus to spread fast (R1=3).
- Sadly, lockdown may not be enough to contain COVID-19. All countries except one seem to have their R1>1. This is a very bad sign.
- Hey, look at Norway! Norway seems to be the only country where its R1<1! And look at the first map I cited. Norway is the only one light orange country among these 13 countries; Mandatory BCG vaccine. To be precise, according to http://www.bcgatlas.org/, Norway had its compulsory BCG vaccine program from 1947 to 2009 for 62 years, which is the longest among these 13 countries.
What are the implications?
- If a country doesn’t have a long history of mandatory BCG vaccination program, lockdown may not be enough to contain COVID-19. Additional measures required. BCG vaccine?
- If a country has a long history of mandatory BCG vaccination program even if it is BCG Denmark strain, a country can contain COVID-19 by the lockdown.
(Added on 2 Apr)This analysis is done by my deep-learning machine, “Enpitsu Namename”. So not explainable. Just for your reference.
- BCG can reduce the infection rate by half no matter what strain is.
- Lockdown can reduce the infection rate to 40%.
- What BCG strain matter seems to be in the death rate. While weak strains such as BCG Denmark may not so effective to reduce the death rate, strong strains such as BCG Tokyo can reduce the death rate to one-tenth.
Below is a table for decision making for each country. Healthcare capacity varies by country but I guess in terms of relative death rate below, 5 to 15 would be the maximum capacity.
| Relative infection rate (No BCG and Ordinary life = 100) | Relative death rate / population (No BCG and Ordinary life = 100) | |||
| Ordinary life | Lockdown | Ordinary life | Lockdown | |
| No BCG | 100 | 40 | 100 | 40~ |
| Mandatory BCG with weak strain (Denmark, etc.) | 50 | 20 | 25~50 | 10~20 |
| Mandatory BCG with strong strain (Tokyo, etc.) | 50 | 20 | 5 | 2 |
I would like to emphasize that BCG strain may matter very much. I have seen a few medical institutions have started to try BCG vaccination against the coronavirus. But I have not seen any medical institution mentioning about the strains. Please try some strains and include strong strains such as BCG Tokyo.
(Added on 3 Apr)I read the following tweet/article.
Probably the most exhaustive and most accurate estimate of COVID-19’s lethality at this time. After correcting for data censoring errors and demographic differences, the overall result is 1.38%. A very important implication is that elaboration of treatment does not appear to have much effect on this figure.
https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(20)30243-7/fulltexthttps://twitter.com/idesan/status/1245052664502726656?s=12
Coincidentally, the result is the same as my deep-learning analysis. From my deep-learning analysis, the death rate (no BCG & Ordinary life) was estimated at 1.38%! And BCG Tokyo reduces it to around 0.1%.
I hope medical experts all over the world examine this hypothesis. I hear that developing a new vaccine will take two years but the BCG vaccine is already here. (Added on 2 Apr) If BCG vaccination works for all including people infected, drive-through BCG vaccination can be a quick and real solution for the U.S. Instead of drive-through PCR testing.
BCG Russia/Tokyo/Brazil looks promising. BTW, I had worked at the Tokyo office of Boston Consulting Group, which is called BCG Tokyo 🙂
Source: jsatonotes.com
The Mazatlan Post


